Analysis of Observations and Measurements in
Clinical, Medical, and Pharmaceutical Business
Observations and Measurements
Many computer systems record information about objects in the real world.
This
information finds its way into computer systems as records,
attributes, objects, and various other representations. The typical route is to
record a piece of information as an attribute to an object. For example, the
fact that a person weighs 185 pounds would be recorded in an attribute of a Person type.
This page examines how this approach fails and suggests more sophisticated
approaches.
We begin by discussing Quantity (Section 1) - a type that
combines a number with
the unit that is associated with it. By combining numbers and units, we
are able
to model the world more exactly. With quantities and their
units modeled as objects, we can also describe how to convert quantities with a
Conversion Ratio (Section 2).
The quantity pattern can be extended by using
Compound Units (Section 3), which represent
complex units explicitly in terms of their components.
Quantities are required for almost all computer systems;
monetary values should always be represented using this pattern.
Quantities can be used as attributes of objects to record information
about
them. This approach begins to break down, however, when there is a very
large
number of attributes that can bloat the type with attributes
and operations. In these situations Measurement (Section 4) can be used
to treat measurements as objects in their own right. This pattern is also useful when you need
to keep information about individual measurements. Here we begin to see the use
of operational and knowledge levels on this page.
Measurements allow us to record quantitative information.
Observation (Section 5)
extends this pattern to deal with qualitative information and thus allows
Sub-typing Observation Concepts (Section 6) in the
knowledge level. It is also often essential to record the Protocol
(Section 7) for an observation so that clinicians can
better
interpret the observation as well as determine the accuracy and sensitivity
of the observation.
A number of small patterns extend observation. The difference between the
time an observation occurred and when it is recorded can be captured with
a Dual
Time Record (Section 8).
Often it is
important to keep a record of observations that have
been found to be incorrect; this requires
a Rejected Observation (Section 9). The biggest headache with observation is dealing with certainty, for it
is often important to record hypotheses about objects. The sub-typing of
Active Observation, Hypothesis, and Projection (Section 10)
is one way of dealing with this problem.
Many statements about observations are made using a process of diagnosis.
We infer observations based on other observations. Associated
Observation (Section 11)
can be used to record the
evidence observations, plus the knowledge that was used
for the diagnosis.
The preceding patterns are structural and are used to make records of our
observations. To understand how they work, it is useful to consider the
Process
of Observation (Section 12),
which can be
modeled with an event-based technique.
Few professions have such complex demands on measurements and
observations as medicine.
The ideas here can be transplanted to other areas: see
Analysis of Corporate Finance page.
Key Concepts
Quantity, Unit, Measurement, Observation, Observation,
Concept,
Phenomenon Type, Associative Function, Rejected Observation,
Hypothesis.
1. Quantity
The simplest and most common way of recording measurements in current
computer systems is to record a number in a field designed
for a particular measurement, such as the arrangement shown in Figure 1. One
problem with this method is that using a number to represent a person's height
is not very appropriate. What does it mean to say that someone's height
is 6, or that someone's weight is 185?
Figure 1 Number attribute.
This approach does not specify the units.
To make sense of the number, we need units. One way of doing
this is to introduce a unit into the name of the association (for example,
weight in pounds).
The unit clarifies the meaning of the number, but the
representation remains awkward. Another problem with this technique is that the
recorder must use
the correct units for the information. If someone tells us their weight is 80
kilograms, what am we to record? Ideally a good record, especially in medicine, records exactly what was measured--no more, no
less. A conversion,
however deterministic, does not follow that faithfully.
In this context a very useful concept is that of quantity. Figure 2
shows an
object type that combines
number and units, for example, 6 feet or 180 pounds.
Quantity includes appropriate arithmetical and comparative
operations. For example, an addition operation allows quantities to be added
together as easily as numbers but checks the units so that 34 inches are not added
to 68 kilograms. Quantity is a "whole value" [2] that the user interface can
interpret and display (a simple print operation can show the number and the unit). In
this way quantity soon becomes as useful and as widely used an attribute as
integer or date.
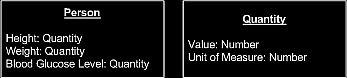
Figure 2 Measurements as attributes using quantity.
Quantity should always be used where units are required.
Example:
We can
represent a weight of 185 pounds as a quantity with Value of 185 and
Unit
of pounds.
Monetary values should also be represented as quantities
(we can use the type
money),
using a currency as the unit. With quantities you can easily
deal with multiple currencies,
rather than being tied to a single currency.
Money objects can also control the representation of
the amount.
Often rounding problems occur in
financial systems if floating point
numbers are used to represent monetary values;
monetary quantities can enforce the use of fixed point numbers for the Value
attribute.
The use of quantity is an important feature of object-oriented analysis.
Many
modeling approaches make a distinction between attributes and
associations.
Associations link types in the model, and attributes contain
some value according to some attribute type. The question is, what makes
something an attribute rather than an association? Usually attributes are the typical
built-in types of most software environments (integer, real, string, date, and
so on. Types such as quantity do not fit into this way of choosing between
attribute and association.
Some
modellers say quantity should be modeled with an association (because it is not a
typical built-in type), while other modellers recommend an attribute (because
it is a self-contained, widely used type). In conceptual
modeling it doesn't really matter which way you do it, the important thing is
that you look for and use types such as quantity. Since we don't distinguish between
attributes and mappings, we don't get into this argument.
(We are laboring this point because we find types such as quantity conspicuously
absent from most of the models we see.)
Modeling Principle
When multiple
attributes interact with behavior that might be used
in
several types, combine the attributes into a new fundamental type.
2.
Conversion Ratio
We can make good use of units represented explicitly in the model. The
first
service that units can perform is to allow us to convert
quantities from one unit to another. As shown in Figure 3 we can use conversion ratio
objects between units and then give quantity an operation, ConvertTo (Unit) ,
which can return a new quantity in the given unit. This operation looks at the
conversion ratios to see if a path can be traced from the receiving object's
quantity to the desired quantity.

Example:
We can convert between inches and feet by defining a
conversion ratio from feet
to inches with the number 12.
Example:
We can convert between inches
and millimeters by defining a conversion ratio
from inches
to millimeters with the number 25.4.
We can then combine this ratio with the conversion ratio from feet to inches to
convert from feet to millimeters.
Conversion ratios can handle most but not all kinds of conversion. A conversion from Celsius to Fahrenheit requires a little more than simple
multiplication.
In this case an individual instance method is required (See
Analysis of Inventory
and Accounting).
If we have a lot of different units to convert, we can consider holding
the dimensions of a unit. For example, force has dimensions of mass times
acceleration,
and force has an S.I. unit of newton, and we also
need a scalar for units that are not S.I. units.
With the dimensions and the scalar,
we can
compute conversion ratios automatically, although it is a bit of work to set it
up.
Be aware that time does not convert properly between days and months
because the number of days in a month is not constant.
If we have several alternative paths in conversion, we can make use of
them
in our test cases. The tests should check that the conversions work in
both
directions.For monetary values, whose units are currencies, the conversion ratios
are
not constant over time. We can deal with this problem by giving the
conversion
ratios attributes to indicate their time of applicability.
When converting between units, we can use either conversion ratios, as
described here, or scenarios
(See
Analysis of Exchange Trading Business).
We use scenarios if the
conversions change frequently and we need to know about many sets of consistent
conversions.
Otherwise, the simpler conversion ratio is the better model.
3. Compound Units
Units can be atomic or compound. A compound unit is a combination of
atomic
units, such as feet or meters per
second. A sophisticated conversion operation can
use conversion ratios on
atomic units to convert compound units. The compound
units
need to remember which atomic units are used and their powers.
Figure 4 is an example of a straightforward model that can convert compound
units.
Remember that the power can be positive or negative.
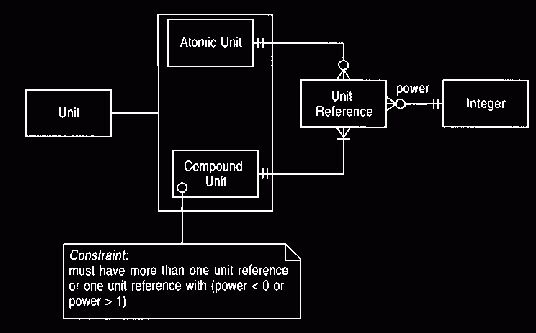
Figure 4 Compound units.
This model can be used for
acceleration and similar phenomena
Example
We can represent an area of 150
square yards by a quantity whose number is 150
and whose
unit is a compound unit with one unit reference to feet with power 2.
A variation on this model takes advantage of representing mappings with
bags. Unlike the usual sets,
bags allow us to use an object more than once in a
mapping, as shown in Figure 5. Bags are particularly useful
when we have a relationship that has a single numeric attribute.
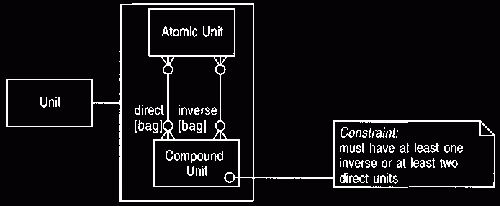
Figure 5 Compound units using bags.
This
model is more compact than
Figure 4
Example
The acceleration due to gravity
can be expressed as a quantity with number 9.81
and a
compound unit with direct units of meter and inverse units of seconds and
seconds.
The difference between Figures 4 and 5 is not great. There's a mild
preference for Figure 5 because it avoids unit reference - a type that
does not do
much.
The choice between these models does not matter to most clients of a compound
unit.
Only clients that need to break the compound unit down into atomic units are
involved, and most of the type's clients would only need some printing
representation.
Obviously we must use Figure
4 if our
method does not allow bags in mappings.
4. Measurement
Modeling quantities as attributes may be useful for a single hospital
department
that collects a couple of dozen measurements for each
in-patient visit.
However, when we look across all areas of medicine, we find thousands of
potential measurements that could be made on one person.
Denning an attribute for each measurement would mean that one person could have
thousands of operations--an untenably complex interface.
One solution is to consider all the various things that can be measured (height,
weight, blood glucose level, and so on) as objects and to introduce the object
type
phenomenon type, as shown in Figure 6. A person would then have many
measurements, each assigning a quantity to a specific phenomenon type.
The person would now have only one attribute for all measurements, and the
complexity of dealing with the measurements would be shifted to
querying thousands of instances of measurement and phenomenon type. We could now
add further attributes to the measurement to record such things as who did it,
when it was done, where it was done, and so on.
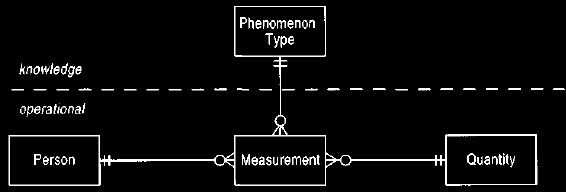
Figure 6 Introducing measurement and phenomenon type.
This model is useful if a large number of possible
measurements would make person too
complex.
The phenomenon types are things we know we can measure. Such knowledge is at the
knowledge level of the model.
Example
John Smith is 6 feet tall,
which can be represented by a measurement whose
person is John Smith, phenomenon
type is height, and quantity is 6 feet.
Example
John Smith has a peak
expiratory flow rate (how much air can be blown out of the
lungs, how
fast) of 180 litres per minute.
This can be represented as a
measurement whose person is John Smith, phenomenon type is peak
expiratory flow rate,
and quantity is 180 litres per minute.
Example
A sample of concrete has a
strength indicated by a force of 4000 pounds per
square inch.
Here the person is replaced by a concrete sample with a measurement whose
phenomenon type is strength and quantity is 4000 pounds per square inch.
This model has a simple division that was found to be very useful in
later
analysis. Measurements are created as part of the day-to-day operation of
a system
based on this model. Phenomenon types, however, are created
on a much more infrequent basis because they represent the knowledge of what
things to measure.
The two-level model was thus conceived: the operational
level consists of the measurement, and the knowledge level consists
of the phenomenon type.
Although it does not seem important in this simple example, we will see that
thinking about these two levels is useful as we explore modeling more deeply.
(Although Figure 6 shows the dividing line, we have left it out of most of the
following figures; however, we have a convention of drawing knowledge concepts toward the top of the figure.)
Modeling Principle
The operational level has those
concepts that change on a day-to-day
basis.
Their configuration is constrained by a knowledge level that changes much less
frequently.
Modeling Principle
If a type has many,
many similar associations,
make all of these
associations objects of a new type.
Create a knowledge level type to differentiate between them.
We could choose to add the unit of measurement to the phenomenon type and
use numbers instead of quantities for the measurement. We prefer to keep
quantities
on the measurement so that we can easily support multiple
units for a phenomenon type.
A set of units on a phenomenon type can be used to check the unit of an entered
measurement and to provide a list for users to choose from.
5. Observation
Just as there are many quantitative statements we can make about a
patient, there
are also many important qualitative statements, such as
gender, blood group, and whether or not they have diabetes. We cannot use attributes
for these statements because there is such a large range of possibilities, so a
construct similar to that for measurement is useful.
Consider the problem of recording a person's gender, which has two
possible
values: male and female. We can think of gender as being what we are
measuring,
and male and female are two values for it, just as any
positive number is a meaningful value for the height
of a person. We can then devise a new type, category observation, which is similar to measurement
but has a category instead of quantity, as shown in Figure 7.
We can also devise another
new type
of observation that acts as a super-type to a measurement and
a qualitative observation.
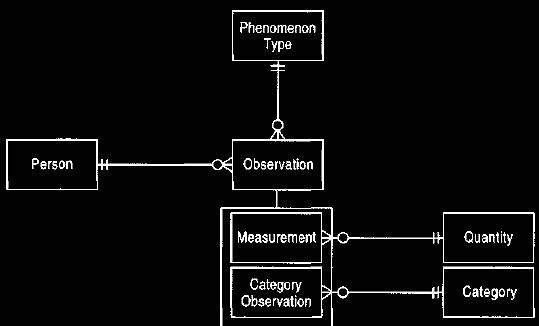
Figure 7 Observations and category observations.
This model supports qualitative measurements, such as blood
group A.
Using Figure 7, we can say that gender is the instance of phenomenon
type,
and male and female are instances of category.
To record that a person is male,
we create an
observation with a category of male and a phenomenon type of gender.
We now have to consider how we can record that certain categories can be
used only for certain phenomenon types. Tall, Average, and Short might be
categories for the phenomenon type height, while A, B, A/B,
and O might be categories for the phenomenon type blood group. This could be
done by providing a relationship between category and phenomenon
type. The interesting question then is the cardinality of the mapping from
category to phenomenon type. We might ask, does the object A used in blood group
potentially link to more than one phenomenon type? One answer is, of course it
does: We grade liver function on the Childs-Pugh scale, which has values A
(reasonable), B (moderate), and C (poor). This raises the question of what we
mean by A. If we mean merely the string consisting of the character 'A,' then
the mapping is multi-valued and the category is independent
of the phenomenon type.
The category's meaning is only clear when a phenomenon type is brought in
through a qualitative observation. The alternative is to make the mapping single-valued, where the category is only
defined within the context of the phenomenon type; that is, it is not A but
blood group A.
What difference is this to us? The single-valued case allows us to record
useful information about the categories, such as A is better than B with
respect to
liver function, while no such ordering exists for blood
groups.
Initial investigations of the clinical process reveals a common sequence:
a patient comes to the facility, evidence is collected about the
patient's
condition,
and a clinician makes an assessment. For example, a patient might come in
complaining of excessive thirst, weight loss, and frequent urination (polyuria).
This would lead a clinician to diagnose diabetes. A couple of things are
important about recording this diagnosis. First, it is not sufficient simply to
note that the patient has diabetes; the clinician must also
explicitly record the evidence used to come up with this diagnosis. Second, the
clinician does not make this kind of deduction out of thin air. Random evidence
is not assembled into random deductions. The clinician must rely on clinical
knowledge.
Consider placing this process in the model we have so far. The patient is
suffering from weight loss.
We can capture this by saying that there is a phenomenon
type of change in weight, with linked categories of gain, loss, and steady.
Similarly there is a phenomenon type of diabetes with categories of present and
absent.
Clearly we can record the link between the observations by placing a
suitable recursive relationship on observation, as shown in Figure 8.
We can thus record the link between the observation of
diabetes and its evidence. We also need to record the clinical knowledge of the
link between weight loss and diabetes. Using the model shown in Figure 7, we would
have difficulty recording this link. The phenomenon type of change in weight and
the category of loss are only linked when an observation is made. We need
a way to say that weight loss, which can exist without any observations, is at
the knowledge level. Making the mapping from category to phenomenon type
single-valued provides the way. (Section 11 discusses this further.)
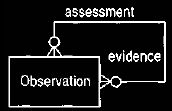
Figure 8 Recursive relationship to record evidence and assessment.
This was the compelling evidence for making the mapping from category to
phenomenon type
single-valued. It moved category to the knowledge level and
renamed it phenomenon, as shown in Figure 9. Phenomena
define the possible values for some phenomenon type.
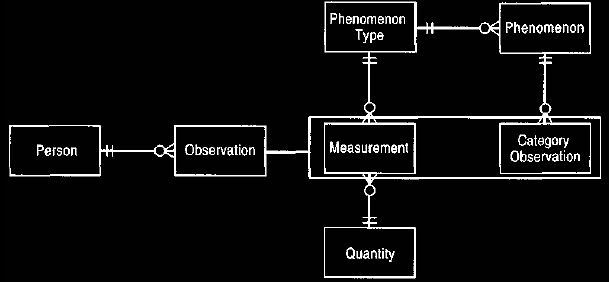
Figure 9 Phenomenon (formerly category) in the knowledge level.
Placing qualitative statements (such as blood group A) in the
knowledge level allows them
to be used in rules.
Example
The fact that a person is blood
group A is indicated by a category observation of a
person whose
phenomenon is blood group A.
The blood group A phenomenon is linked to the phenomenon type of blood group.
Example
We can model a low oil level in
a car as a category observation of the car. The
phenomenon
type is oil level with possible phenomena of over-full, OK, and low.
The observation links the car to the low phenomenon.
The model in Figure 9 works well for category observations with several
values for a phenomenon type. But many observations involve merely a
statement
of absence or presence rather than a range of values.
Diseases are good examples of these: Diabetes is either present or absent. We
could use Figure 9 with the phenomena diabetes absent and diabetes present. This ability
to explicitly record the absence of diabetes is important, but it may also be
sensible to record absence of weight loss. (If a patient comes in with symptoms of
diabetes but has not been losing weight, then that would contra-indicate
diabetes. This does not imply that the weight is increasing or steady, merely that it is not
decreasing.) Indeed we can record the absence of any phenomenon, particularly to
eliminate hypothetical diagnoses.
Thus the
model shown in Figure 10 allows any category observation to have
presence and
absence. Observation concept is added as a super-type of
phenomenon.
This is done to allow diabetes to be an observation concept without attaching it
to some phenomenon type.
Example
We record the fact that John
Smith has diabetes by a presence observation of
John Smith linked to the
observation concept diabetes.
Example
We represent spalling
(deteriorating) concrete in a tunnel by an observation with
the tunnel
instead of the person, and an observation concept of spalling concrete.
We also need a feature on the observation to indicate where in the tunnel the
spalling occurs.
(Medical observations may also need an anatomical location for some observation
concepts.)
6. Sub-typing Observation Concepts
Figure 10 introduces a super-type relationship that allows
generalization of
observation
concepts. This is quite common in medicine and is valuable because observations can be made at any level of generality. If an
observation is made of the presence of the sub-type, then all super-types are also
considered to be present.
However, if an observation is made of the absence of a
sub-type, then that implies neither presence nor absence of super-types.
Observation of absence does imply all sub-types are also absent. Thus presence is propagated up the
super-type hierarchy, while absence is propagated downward.
Example
Diabetes is an observation
concept with two sub-types: type I diabetes and type II
diabetes. An
observation that type I diabetes is present for John Smith implies that diabetes is also present for John Smith.
Example
Blood group A is called
polymorphic because it can be sub-typed to A1 and A2.
The other blood groups are not
polymorphic.
7. Protocol
An important knowledge concept for recording observations is the
protocol-- the
method by which the observations were made. We can measure a
person's body temperature by placing a thermometer in the mouth, armpit, or
rectum. Usually the temperature readings these techniques yield can be
considered the same; nonetheless, it is vital to record which approach we used. A
strange observation can often be explained by understanding the technique that
was used to reach it.
Thus in health care it is accepted practice to always record
what tests are used to record observations.
One of the values of a protocol is that it can be used to determine the
accuracy and
sensitivity of a measurement. This information could be recorded
on the
measurement itself, but usually it is based on the protocol that is used for
the observation. Holding it at the protocol makes it easier
to capture this information.
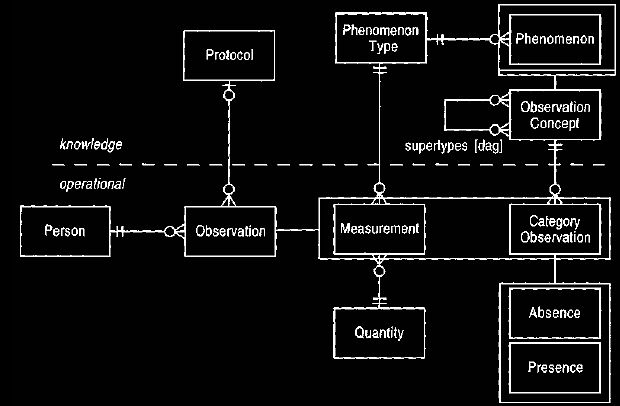
Figure
10
Absence and presence of observation concepts.
The absence of a phenomenon can be as valuable as finding a
presence.
8. Dual Time Record
Observations often have a limited time period during which they can be
applied.
The end of the time period indicates when the observation is
no longer applicable.
This time period is different than the time at which the
observation is made. Thus there are two time records (which may be periods or
single time points) for each observation: one to record when the observation is applicable
and the second when it is recorded, as shown in Figure 11.
Example
At a consultation on May 1,
2008, John Smith tells his doctor that he had chest
pain six
months ago that lasted for a week.
The doctor records this as an observation of the presence of the observation
concept chest pain. The applicability time record is a time period starting at
November 1, 2007 and
ending at November 30, 2007. The recording time is the time-point May 1,2008.
(Note that some way of recording approximate time-points would be valuable
here.)
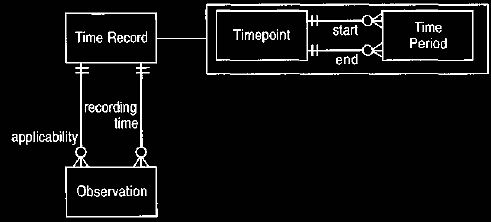
Figure 11 Dual time record for observation.
A time record allows both
periods and single points to be recorded. Most events have a
separate occurring and recording time
9. Rejected Observation
Inevitably we make mistakes
when making observations. In the case of medical
records, however, we cannot just erase them. Treatments may
have been based on these mistakes, and there are usually legal restrictions. To
handle this consideration, we can classify observations as rejected observations
when it is found that they were and are untrue, as shown in Figure 12.
(Note the difference between this and an observation that was true but is no
longer true, such as a healed broken arm. A healed broken arm is never rejected, but
its applicability time record is given an end date.) Rejected observations must
be linked to the
observation that rejects them.

Figure 12 Rejected observations.
Observations cannot be deleted if a full audit trail is
needed.
Example
John Smith has a blood test
that indicates a large mean corpuscular volume. This
can be due
to either pernicious anemia or alcohol abuse.
John Smith informs the doctor that he drinks very little alcohol. This indicates
the presence of pernicious anemia, which leads to further tests and treatment.
Six months later it is discovered that John Smith drinks heavily. This
information indicates that the observation of pernicious anemia should be
rejected by an observation of alcohol abuse. The rejected
observation of pernicious anemia must be retained to explain the treatment that
ensued.
10. Active Observation, Hypothesis, and
Projection
As observations are
recorded, many levels of assurance are given. A clinician
might be
faced with a patient showing all the classic symptoms of diabetes.
The clinician records that she thinks the patient probably has diabetes, but she
cannot be certain until a test is done, and in many diseases even a test does
not provide 100 percent certainty. One approach to recording this kind of
information is to assign probabilities to observations, but this method is
unclear and does not seem natural. The alternative is to use two classifications:
active observation and hypothesis, as shown in Figure 1 The distinction is
subtle: An active observation is one that the clinician "runs with," probably
using it as a basis for treatment. A hypothesis more likely leads to further
tests.

Figure 13 Active observation, hypothesis, and projection.
Example
A patient with observations of the presence of
thirst, weight loss, and polyuria
indicates diabetes. With just these symptoms, however,
a clinician makes a hypothesis of diabetes and orders a measurement of the
fasting blood glucose. The result of this test
indicates whether to confirm the hypothesis or reject it.
Both sub-types, active observation and hypothesis, represent observations
of
the current state of the patient. Projections are observations that the
clinician
thinks might occur in the future. Often clinicians decide on
treatments by considering future conditions that may occur. If the prediction is
true, it is recorded with an additional active observation.
Example
If a patient has rheumatic fever, or consequent
rheumatic valve disease, there is a
risk
of endocarditis. This risk is recorded as a projection of endocarditis.
Treatments will then be based on this projection.
The certainty of observations is one area of much discussion.
The final model reflects the clinicians' views of what was
the most natural.
The classic approach of assigning probabilities might make sense to science
fiction aficionados, but it clearly did not to clinicians (who could predict
asking questions such as "What are we to make of the difference between 0.8 and
0.7?"). With active observation and hypothesis, the final concept is more clear,
although the choice of which classification to use is more problematic. In the end
only the group of experienced clinicians can make a useful decision on this area in an almost
instinctive way. The professional analyst can only point out
some formal consequences.
11. Associated Observation
At this point we can look at
ways to record the chain of evidence behind a
diagnosis. The basic idea is to allow observations to be linked to each other
(the patient's thirst indicated the patient's diabetes) and
observation concepts to be so linked (thirst indicates diabetes). Thus we see
that the knowledge and operational levels are reflections of each other, as shown in Figure
14. These reflections are linked by associations that show how knowledge
concepts are applied to the operational level. In this case the links occur not only
between the observation and the observation concept but also between the
evidence conclusion links. Thus when we say the patient's thirst indicates that the patient
has diabetes, we are making use of, and should explicitly record that we are
making use of, the general connection between thirst and diabetes. Figure 14 shows how
we make types to hold not just observations and observation concepts but also
types for the links at the operational (associated observation) and the knowledge
(associative function) level.
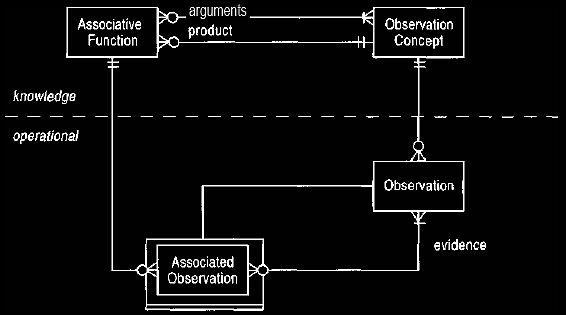
Figure 14 Links between observations.
Actual evidence chains for a patient are recorded at the
operational level. The knowledge
level describes what chains are
possible.
Example
A clinician observes weight
loss, thirst, and polyuria in a patient and makes an
associated
observation (and hypothesis) of diabetes based on the evidence observations.
The associated observation is linked to an associative function whose arguments
are the observation concepts--weight loss, thirst, and polyuria - and whose
product is diabetes.
Example
If our car does not start and
the lights do not work, then both of these observations are evidence for the
associated observation of a dead battery. Car not starting, lights not working, and dead battery are all observation
concepts linked by an associative function.
Note that the knowledge and operational levels are not complete mirror
images of each other. Associated observation is a sub-type of observation,
but
associative function is not a sub-type of observation concept.
It seemed natural to make associated observation a sub-type of observation since,
at the operational level, one particular observation is made with supporting
evidence. At the knowledge level, the rule with arguments and conclusion is
recorded. One observation concept may have several associative functions
for which it is the result, but a particular observation has only one set of
observations as evidence.
12. Process of Observation
This section has concentrated on the static elements of observation: what
an
observation or measurement is and how we can record it in a
generic way to support the analysis that clinicians need to perform on it.
It is significant that in modeling we found that we could conceive of a general
static model, but the behavioral part was much more dependent on individual
departments. Of course, a static model implies a great deal of behavior.
Behaviors exist to create observations and to provide various ways of navigating
associations to understand how those observations fit with other observations.
The behavior we cannot imply, however, is the sequence of observations that a typical
department makes. Often a clinician has some path of observations that can be
taken. Departmental policy may be to record this path in terms of higher-level protocols
(see Analysis of Planning
of Business>).
It is
difficult, and almost certainly impossible, to design a general process
that all
clinicians could use.
It is possible, however, to sketch an outline of the process involved in
making
observations. We begin by
looking at how making a new observation can trigger
further observations, as shown in Figure 15. Whenever
clinicians make observations, they consider the possibility of other associated
observations.
They use the associative functions they know to come up with a list of possible
observation concepts that might be associated with the triggering observations.
They can then propose further observations as needed.
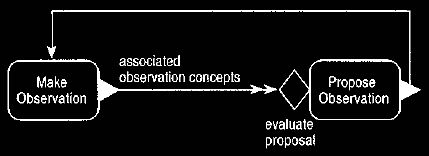
Figure 15 Making an observation triggers further
observations.
Further observations are suggested by the knowledge level.
In Figure 15 the concurrent trigger rule is labelled "associated
observation
concepts." In event diagrams, trigger rules have two purposes. First,
they show
cause and effect. When we are considering business processes,
this is usually enough, but as we delve deeper we see a second purpose. Any
operation has input and output. The trigger that connects two operations must
describe how to get from the output of the triggering operation to the input of
the triggered operation.
In many cases this is trivial, as they are the same object
(as in the trigger from propose observation to make observation shown in Figure
15). However they can get quite complex, as in finding associated observation
concepts.
When we have a more complex trigger rule, we can represent the
trigger rule
with another event diagram.
Figures 16 and 17 do this for the associated
observation concepts trigger. We begin by finding all the
associative functions whose input includes the initial observation's observation
concept. We then evaluate each of these associative functions. For each one
that evaluates to true, we find the product and add it to the answer. Since
these event diagrams describe a trigger rule query, all the operations must be accessors and
hence must not change the observable state of any object.
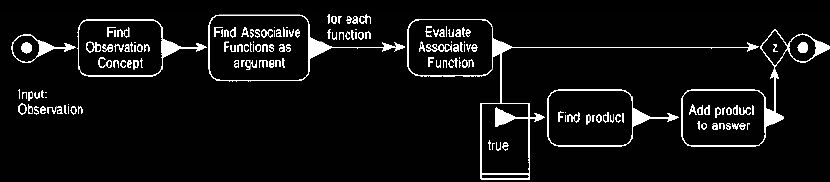
Figure 16 Event diagram to describe the query for finding
associated observations.
This lies on the concurrent trigger of Figure 15 or in the
operation of Figure 18.
When the trigger rule query
is complex, you can also represent the query as an operation in its own right,
as shown in Figure 18. Either method is correct.
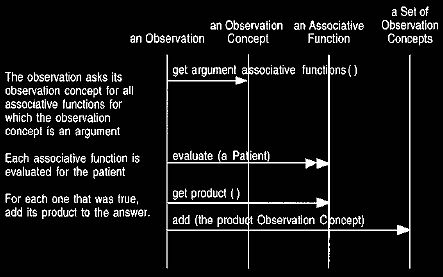
Figure 17 An interaction
diagram for finding the possible observation concepts implied
by
an observation.
This interaction diagram supports Figure 16.

Figure 18 Notating the query explicitly as an operation.
This is equivalent to Figure 15. You can either show
queries as operations or consider
them part of the trigger, trading simplicity for compactness.
Even after the query, there is a control condition (evaluate proposal)
before
an observation is proposed. The query suggests possible observation
concepts to
look for based on the associative functions. This step could
easily be done by software in a decision support system. The control condition
represents the extra step of deciding whether the suggested observation concept is
worth testing for. We did not feel we could formally model this process,
implying that this step is beyond software and can only be done in the clinician's head.
Figure 19 includes additional triggers that arise from projections and
active observations. The triggers to propose intervention work in a
similar way
to the previous case. We suggest interventions that are
evaluated by the clinician before they are proposed. This reinforces the fact
that although any observation can lead to further observations being made, only
active observations or projections (not hypotheses) lead to interventions.
(An intervention
is an action which either
intends or risks a change in state of the patient.)
The
trigger queries work in a similar way with the knowledge
level but involve start functions, which are discussed briefly in
Planning of Business,
Section 7.
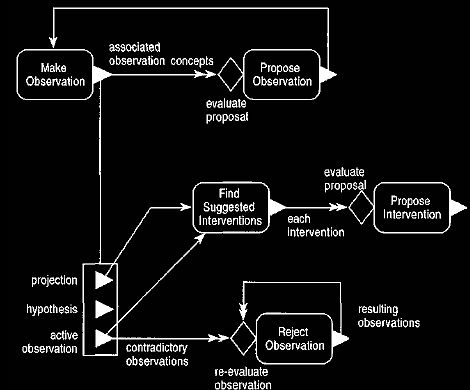
Figure 19 Event diagram for the process of working with
observations. This
extends Figure 15 with similar triggers for interventions
and rejections.
The final trigger on Figure 19 shows how the appearance of an active
observation can contradict other observations and thus lead to those
observations
being rejected. Again this can involve associative functions,
but this time we are looking for a contradiction. Once an observation (which may
be a hypothesis) is rejected, further observations which were supported by this
observation must be reconsidered.
One of the interesting things about the work that produced these patterns
is
the way the abstractions
were found. Although the final results discussed here are
usually structural, behavioral modeling played a central role
in understanding how the concepts worked. The fact that clinicians did the
modeling themselves was also crucial.
The abstraction of observation is central to these patterns; it ties together
signs, symptoms, and diagnoses, which clinicians have long considered to be very
different.
It was only by going through the modeling process that clinicians could pull out
the abstraction.
If software engineers had come up with such an abstraction, we doubt if they
could ever convince clinicians that it was valid.
And there would be good reason to be doubtful, since software engineers can
never have that deep knowledge of medicine.
The best conceptual models are built by domain experts, and they are often the
best conceptual modellers.
|